
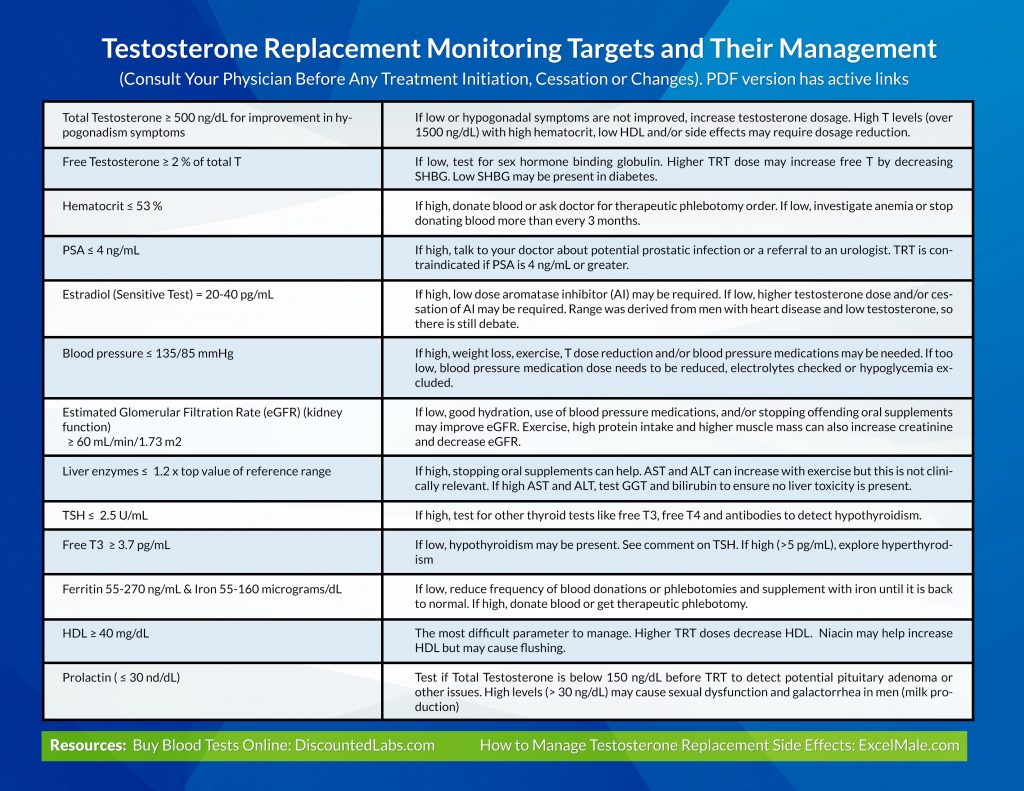
Testosterone Replacement Monitoring Targets and Their Management
(Consult Your Physician Before Any Treatment Initiation, Cessation or Changes).
| Total Testosterone ≥ 500 ng/dL for improvement in hypogonadism symptoms | If low or hypogonadal symptoms are not improved, increase testosterone dosage. High T levels (over 1500 ng/dL) with high hematocrit, low HDL and/or side effects may require dosage reduction. |
| Free Testosterone ≥ 2 % of total T | If low, test for sex hormone binding globulin. Higher TRT dose may increase free T by decreasing SHBG. Low SHBG may be present in diabetes. |
| Hematocrit ≤ 53 % | If high, donate blood or ask doctor for therapeutic phlebotomy order. If low, investigate anemia or stop donating blood more than every 3 months. |
| PSA ≤ 4 ng/mL | If high, talk to your doctor about potential prostatic infection or a referral to an urologist. TRT is contraindicated if PSA is 4 ng/mL or greater. |
| Estradiol (Sensitive Test) = 20-40 pg/mL | If high, low dose aromatase inhibitor (AI) may be required. If low, higher testosterone dose and/or cessation of AI may be required. Range was derived from men with heart disease and low testosterone, so there is still debate. |
| Blood pressure ≤ 135/85 mmHg | If high, weight loss, exercise, T dose reduction and/or blood pressure medications may be needed. If too low, blood pressure medication dose needs to be reduced, electrolytes checked or hypoglycemia excluded. |
| Estimated Glomerular Filtration Rate (eGFR) (kidney function)
≥ 60 mL/min/1.73 m2 |
If low, good hydration, use of blood pressure medications, and/or stopping offending oral supplements may improve eGFR. Exercise, high protein intake and higher muscle mass can also increase creatinine and decrease eGFR. |
| Liver enzymes ≤ 1.2 x top value of reference range | If high, stopping oral supplements can help. AST and ALT can increase with exercise but this is not clinically relevant. If high AST and ALT, test GGT and bilirubin to ensure no liver toxicity is present. |
| TSH ≤ 2.5 U/mL | If high, test for other thyroid tests like free T3, free T4 and antibodies to detect hypothyroidism. |
| Free T3 ≥ 3.7 pg/mL | If low, hypothyroidism may be present. See comment on TSH. If high (>5 pg/mL), explore hyperthyrodism |
| Ferritin 55-270 ng/mL & Iron 55-160 micrograms/dL | If low, reduce frequency of blood donations or phlebotomies and supplement with iron until it is back to normal. If high, donate blood or get therapeutic phlebotomy. |
| HDL ≥ 40 mg/dL | The most difficult parameter to manage. Higher TRT doses decrease HDL. Niacin may help increase HDL but may cause flushing. |
| Prolactin ( ≤ 30 nd/dL) | Test if Total Testosterone is below 150 ng/dL before TRT to detect potential pituitary adenoma or other issues. High levels (> 30 ng/dL) may cause sexual dysfunction and galactorrhea in men (milk production) |
You can buy all of these tests by clicking on this panel and adding other tests in the drop down menu: TRT MALE Hormone/Wellness Follow Up Panel
It is also important to learn how to prevent and manage testosterone replacement side effects: ExcelMale.com

")











{kind=link}